Overview & Background: Definition Of Immunogenicity
Immunogenicity assessments are an integral component of the drug discovery and development process. But what does immunogenicity mean? It is the characteristic of a foreign substance responsible for provoking an immune response. In recent years, we have witnessed the emergence of Mesoscale Discovery Electrochemiluminescence (ECL) multi-array platform for MSD bridging immunogenicity ADA antidrug antibody assay development and cell-based neutralizing antibody assay development. These immunogenicity assessment assays are highly sensitive and provide a broader dynamic range along with a higher therapeutic tolerance as measured in PK ADA analysis. Our veteran scientists at NorthEast Bioanalytical Laboratories are always prepared to develop and validate your ADA and NAb assays for subsequently performing immunogenicity assessment in your preclinical and clinical study ADA samples.
Immunogenicity Assay Platforms
As immunogenicity testing is necessary throughout the drug development life cycle, one must have access to robust platforms and facilities for reliable pharmacokinetics or PK ADA antibody results. NorthEast BioLab is a full-fledged ADA lab and offers top-quality ADA services using several technologies, including Mesoscale Discovery Electrochemiluminescence Assays as well as ELISA ADA assay. Furthermore, we are flexible in creating a tailored testing approach for your ADA antidrug antibody assays and NAb assays leveraging our deep expertise in both immunology and drug development.
Immunogenicity Assay Services
Our Mesoscale Discovery immunogenicity assay services include all aspects of your critical reagent preparation, method development, ADA validation, and sample analysis. These services include securing assay reagents, tagging or conjugating reference compounds and antibodies, customizing assay plates, etc.
Immunogenicity Assay Format
Different assay formats are available for ADA assay protocols and processes, including bridging assays, direct binding assays, and soluble-phase binding assays. Each format has its unique advantages and disadvantages. For example, antigens with repetitive motifs may produce false-negative results in bridging assay format. Bridging assays are a type of sandwich ELISA ADA assay, where a bridge is created between a labeled and unlabeled antigen to detect ADA antidrug antibody in the sample. However, the primary difference between each assay format is the number of wash steps that may influence assay sensitivity.
FDA Immunogenicity Guidance
FDA immunogenicity guidance recommends employing a stratified approach to manage more extensive immunogenicity assessment. Here, we must detect low levels of anti-drug antibodies in the preliminary studies. Subsequently, we must assay positive samples to eliminate any false positives. Finally, immunogenicity FDA guidance recommends characterizing anti-drug antibodies for determining assay functionality. Specifically, antibody immunogenicity guidelines mention utilizing the cell-based neutralizing antibody assay principles for thoroughly characterizing anti-drug antibodies.
Strategies For Immunogenicity Assessment
There are three primary strategies for immunogenicity assessment, namely i) multi-tiered approach, ii) immunoglobulin isotypes or subtypes, and iii) domain specificity. Let us explore each of these immunoassay strategies in detail.
Multi-tiered Testing Approach
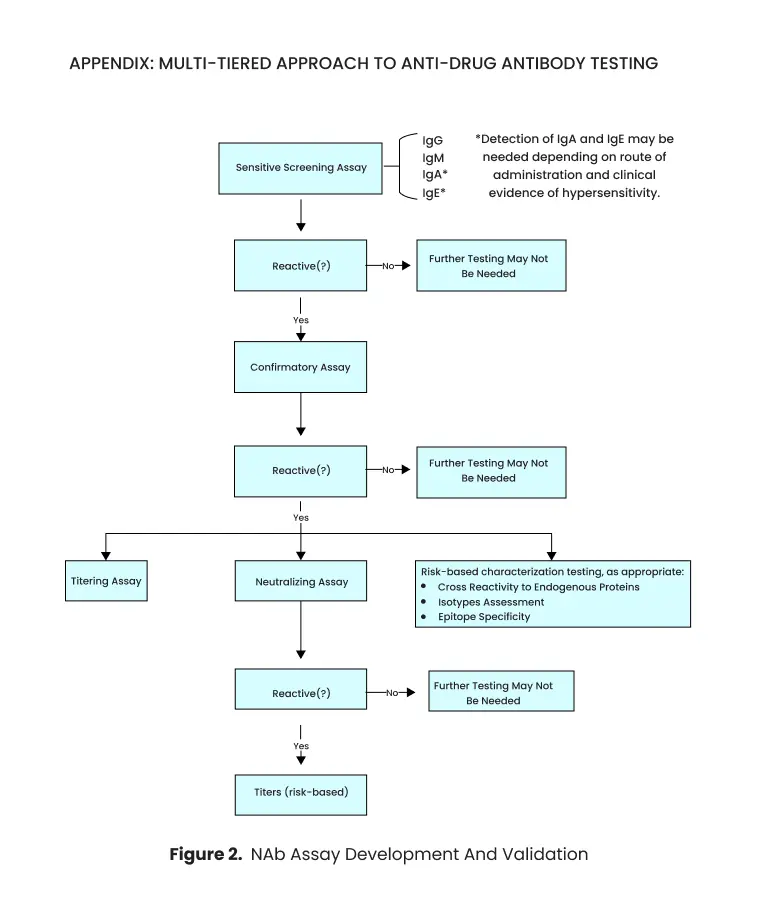
Generally, FDA recommends a multi-tiered anti drug antibody testing approach for immunogenicity assays. In this approach, a primary sensitive screening assay assesses clinical samples. Positive samples from screening assays are exposed to a confirmatory assay. The confirmatory assay helps demonstrate the specificity of Anti Drug Antibodies towards the targeted therapeutic protein. Finally, the positive ADA samples from confirmatory assays get characterized using other approaches, such as neutralization and titration assays. This multi-tiered approach is critical for effective ADA analysis in clinical trials.
Immunoglobulin Isotypes Or Subtypes
The primary screening step must detect all Ig isotypes. When there is no risk of anaphylaxis or for non-mucosal administration of a drug, IgM and IgG are the relevant PK ADA antibody isotypes. However, for mucosal administration, IgA isotypes must also be considered. Notably, FDA expects all relevant isotypes to be detected in the screening assay. In some cases, assessing ADA PK analysis subtypes may provide additional information. Hence, one can evaluate specific subtypes or isotypes of immunoglobulins based on the intended goal. Accurate ADA analysis in clinical trials requires considering all relevant immunoglobulin isotypes and subtypes.
Domain Specificity
Some therapeutic proteins consist of multiple domains. Each of these domains may function in a unique way to elicit clinical efficacy. An immune response mounted against one specific domain may inhibit that particular function but leave the other domains intact. Hence, FDA recommends testing immunogenicity for the entire therapeutic protein. Besides, one must confirm the binding of anti drug antibody to clinically relevant domains. This aspect of ADA analysis in clinical trials ensures comprehensive assessment of the immune response against therapeutic proteins.
Risk-based Immunogenicity
ADA-generated immune responses are highly variable. Therefore, FDA recommends a risk-based approach to evaluate and manage immune responses and clinically relevant adverse events. This approach needs to assess the effects of immune responses on the safety, efficacy, and PK/PD properties of therapeutic drug products. Besides, the immunogenicity test must identify ADAs that can generate unwanted consequences, such as hypersensitivity responses and PK ADA neutralizing antibody activity. Implementing a risk-based approach is essential for thorough ADA analysis in clinical trials, ensuring the safety and effectiveness of therapeutic drug products.
ADA Antibody Assays
NorthEast Bioanalytical Laboratories specialize in performing Antidrug Antibody Assays and Neutralizing Antibody (nAb) Assays for large-molecule antibody therapeutics or proteins that may elicit an immune response in the body. ADA antibody assays detect these drug specific antibodies. However, the generated immune response may range from minor clinical observations to life-threatening interactions. Moreover, the ADA may bind to the drug molecule and neutralize the therapeutic. Besides, this interaction may also cross-react with endogenous molecules. Preclinical and clinical ADA study have shown anti-drug antibodies have significantly induced changes in toxicology, pharmacokinetics, and efficacy. Hence, NorthEast Bioanalytical Laboratories also specialize in neutralizing antibody assays to determine these ADA interactions. We set up rigorous ADA antibody assay protocols for system suitability at each stage of the immunogenicity assessment thus extending our capabilities as a robust ADA CRO
Preclinical Immunogenicity ADA Assays
NorthEast Bioanalytical Laboratories support all aspects of drug development and discovery, including your PK ADA studies. Anti-drug antibody responses observed in preclinical studies may not necessarily correlate with clinical immunogenicity data. However, immunogenicity interactions observed in animal models may help scientists design pharmacology and toxicology studies. Besides, toxicity data derived from preclinical antibody immunogenicity testing may give insights into expected toxicity in subsequent ADA analysis in clinical trials.
Immunogenicity ADA Assays For Clinical ADA Study
Our veteran scientists have vast experience in handling immunogenicity assays for clinical studies via processes such as ADA assay development for immunogenicity testing of therapeutic proteins. Regulatory agencies require the strategy and rationale for clinical ADA trials during the IND phase of drug development. The method for immunogenicity assays must consider the risks of the candidate drug. Usually, large molecule drugs having an endogenous molecule pose higher risks than drugs with unessential endogenous biomolecules. However, one can save patients’ ADA samples and perform ADA PK analysis and drug bioanalysis for lower-risk drugs.
Cut-Point – ADA Screening
The cut-point in ADA screening is crucial for immunogenicity testing. This importance is because the cut-point level determines the positive or negative sample results during anti drug antibody testing. One can define the cut-point level by analyzing naive ADA study subjects. However, the cut-point must consider sample variability among the naive subjects. Also, the cut-point or ADA plate method used depends on several factors, such as statistical outliers, pre-existing antibodies, and interfering factors.
Neutralizing Antibody (NAb) Assays
Confirming whether ADA neutralizes the therapeutic compound is crucial in drug immunogenicity testing. A neutralized drug becomes ineffective against its desired end goal. Most neutralization assays are in-vitro cell-based assays. However, one may also conduct enzymatic activity and ligand binding neutralizing antibody (NAb) assays. NorthEast Bioanalytical laboratories develop and validate ligand-binding, enzymatic activity, and cell-based NAb assays by adhering to the guiding principles and ADA protocols.
Cell-Based Neutralizing Antibody Assays
Cell-based assays are preferred for NAb testing because a thoroughly developed cell-based NAb assay can test multiple functional domains of a drug-protein in a single assay. A large protein therapeutic has multiple-functional domains, and therefore, NAb can potentially bind within these domains and alter drug efficacy. Cell-based NAb assays can detect fluctuations in drug activity and thus confirm whether ADA neutralizes the therapeutic drug.
Ligand Binding Neutralizing Antibody Assays
Sometimes ligand-binding NAb assays are appropriate during immunogenicity testing. Ligand-binding NAbs could be beneficial for certain drugs, such as monoclonal antibodies that could be affected by ADAs.
Enzymatic Activity Neutralizing Antibody Assays
Some protein drug compounds are enzymes. One may measure the activity of these enzyme therapeutics using enzymatic activity NAbs. For these drug products, drug neutralization by ADAs is confirmed if the enzymatic activity of the drug is decreased in the presence of ADA.
nAb Assay Development and Validation
Development of NAb assay development and validation requires a thorough understanding of the drug molecule and is specific to the drug of interest. The mechanism of action and pharmacodynamic properties of the therapeutic must be evaluated before developing NAb assays. Besides, they should identify and characterize all functional domains of the drug compound so that NAb assays could assess individual parts.
Moreover, NAb assay validation must meet all regulatory expectations. The FDA immunogenicity guidance recommends a minimum of 30 samples for NAb analysis. Besides, these samples must be tested on at least three separate days and employ at least two different analysts. Furthermore, all relevant validation parameters, such as specificity, sensitivity, and precision, should be evaluated during assay validation.
Antidrug Antibody Assays Cut-Point
The assay cut-point level defines whether the study sample is positive or negative. Determining assay cut-points is crucial for minimizing the possibility of false-negative readings. Numerous matrix components or interfering products may influence assay cut points. Hence, these components must be tackled early during ADA assay development. As samples from different study samples and disease states may comprise constituents producing varying degrees of background signal, cut-points must be determined for individual populations.
Whenever possible, one must use treatment-naive participants to determine the cut-point statistically. Besides, running the experiment in replicates may help estimate assay variability. The statistical approach for determining assay cut-point may include accounting for pre-existing antibodies and removing statistical outliers.
Antidrug Antibody Assays Sensitivity
ADA analysis in clinical trials necessitates a high level of assay sensitivity to accurately detect antibodies. Assay sensitivity of ADA assay is the lowest concentration of antibody preparation that consistently gives a readout equal to the predetermined cut-point or a positive result. The bioanalytical assay must produce sensitive readings before associating them with altered safety, efficacy, pharmacokinetic or pharmacodynamic profiles. Antibody specificity assay studies comprise positive control (PC) antibody preparations, which may be different from the ADA responses in study subjects.
As assay sensitivity may be affected by the ADA study drug, it is essential to define the sensitivity of the assay in using the concentrations of these specific drugs. US FDA recommends the sensitivity to be at least 100 ng/mL for screening and confirmatory IgM and IgG ADA assays. However, assay sensitivity greater than 100 ng/mL can be considered on a case-to-case basis. Traditionally, the US FDA requires assay sensitivity to be at least 250-500 ng/mL. But recent research suggests that lower concentrations of up to 100 ng/mL can be correlated with ADA Clinical Trial incidents.
ADA Antibody Assay Drug Tolerance, Sensitivity, and Suitability
Blood or serum may have endogenous or dosed components that may influence ADA immunoassay sensitivity. Hence, drug tolerance during ADA assay development is critical for understanding the assay suitability and sensitivity in dosed subjects. Drug tolerance ADA assays are performed using the expected concentrations of interfering free drug or endogenous components. Besides, the US FDA recommends simultaneously performing ADA pharmacokinetics assays early during drug development.
To determine interference with ADA detection, different known concentrations of positive control antibodies must be added in ADA-negative control in the presence or absence of the drug product. Moreover, one must consider factors influencing drug tolerance, such as the nature of the target, assay selectivity, and type of positive control when developing bioanalytical assays.
Specificity Of ADA Antibody Assay
Ensuring the accuracy and reliability of assays in ADA clinical trials is paramount to assessing the safety and efficacy of drug products. A highly specific assay will detect only the target ADA. Hence, issues with assay specificity can generate false-negative results, which may influence the safety and efficacy of the drug product. However, demonstrating antibody assay specificity against responses to Fc-fusion proteins, Ig-fusion proteins, and mAb may be challenging as human serum has higher concentrations of Ig. Therefore, the assay must determine anti-mAb antibodies and exclude the non-specific endogenous antibodies, soluble drug target, mAb product itself, or other assay reagents. Besides, for subjects with a higher rheumatoid factor, it is essential to demonstrate that the assay effortlessly differentiates between antibodies and the rheumatoid factor or that the rheumatoid factor does not affect assay performance.
Antibody specificity is determined by showing that the binding of unlabeled or soluble purified therapeutic protein can be blocked. It is important to demonstrate specificity by incubating negative or positive antibody controls with the therapeutic protein. When the relevant therapeutic protein inhibits the signal, then the response is specific. However, determining the assay specificity of multimeric antibodies is challenging and may require more approaches. Here, another mAb with the same Fc region can be included, which can provide additional data. For a selective and specific ADA assay, introducing the therapeutic compound may reduce the assay signal. However, adding therapeutic compounds may not necessarily influence other antibodies already present in the solution.
Selectivity Of ADA Antibody Assay
Assay selectivity is the characteristic of an assay to identify specific ADAs in the presence of other compounds. Several factors, such as onboard therapeutic drugs or endogenous components in the matrix, may interfere with ADA PK analysis selectivity. Besides, most biological matrices comprise a substantial amount of endogenous proteins, and failure to determine selectivity may give rise to non-specific signals.
Matrix Interference
Understanding matrix interference is a crucial aspect of assay selectivity. Sample matrices such as serum, plasma, and saliva will have some degree of interference. Besides, the signal may be suppressed when comparing matrix versus diluent assay performance. Exogenous and endogenous elements may influence assay results. Therefore, ADA samples must be diluted to minimize these effects. Moreover, they must define the dilution factor and sample matrix before validating ADA assays.
Various matrix components such as lipids, bilirubin, free hemoglobin, and concomitant medications may influence assay results. For example, different anticoagulants will have distinct effects on assay results and potentially affect assay sensitivity. Hence, one can spike different known concentrations of positive control antibodies with both the absence or presence of an ADA study matrix to assess matrix interferences. Although, ADA recovery in the buffer can provide insights into the degree of matrix interference present in the sample.
Minimal Required Dilution
Matrix components can obscure positive assay results. Hence, it becomes necessary to frequently dilute the ADA samples to maintain the ability of the assay to detect ADAs. The MRD has multiple definitions. However, to calculate ADA titer and assay sensitivity, the final sample dilution is considered for MRD.
Validation Of PK ADA Screening Assay
Assay validation is a vital bioanalytical process for demonstrating the suitability of PK ADA assays for their intended use. ADA validation employs specific investigation to assess assay characteristics.
Sensitivity of Screening Assay
All general assay validation considerations are applicable for screening assays. These considerations include fundamental ADA validation parameters such as cut-point, specificity and selectivity, sensitivity and drug tolerance, reproducibility, precision, robustness, and stability. As initial screening results are vital for subsequent sample analysis, sensitivity is crucial at this stage.
Cut-Point of Screening Assay
In ADA clinical trials, it’s imperative to include an appropriate set of treatment-naive subjects for statistically determining the cut-point of screening assays. Besides, two analysts must test each sample on at least three separate days for screening assays. One approach analysts often employ for high assurance of a false-positive rate of 5% is to consider a 90% one-sided lower confidence interval for 95% of the negative control subjects. This approach ensures that the assay identifies all participants developing antibodies.
Other strategies include the use of median absolute deviation and median instead of standard deviation and mean. However, the mean reaction of negative controls may vary between plates or assays. If the mean varies, but variance around the mean doesn’t, a floating cut-point can be used. A floating cut-point is a statistically determined normalization factor applied in certain technical situations.
Selection Of Antidrug Antibody Assays Reagents
Several ADA assay elements are standard and are acquired from commercial sources. However, other components, such as negative controls, positive control antibodies, and system suitability controls, need to be generated specifically for the intended purpose. Hence, the qualification and stability of assay reagents are essential for robust and reliable assay results.
Development of Positive Control Antibodies
For routine maintenance and assay assessments, one can use the same positive controls for validating, developing, and monitoring assay performance. However, for system suitability controls, it is vital to include a positive control antibody to detect hook effects and maintain assay sensitivity. There are different approaches to generating positive controls. Usually, animals are immunized in the presence or absence of adjuvants to generate positive control antibodies. However, the US FDA recommends affinity purifying for the immunized animals with the therapeutic protein in the case of positive control antibodies. This process ensures that the polyclonal antibody preparation is enriched and enables better interpretation of assay results.
Notably, one must take utmost care while choosing animal species. Although, when the positive control antibody is undetectable, including a positive control for the secondary reagent is necessary so that the reagents perform as intended.
Development of Negative Controls
FDA recommends developing negative controls for subject sample testing and validation studies. Sera from a set of treatment-naive subjects can be used as negative controls. However, the value obtained should be close but lower than the predetermined cut-point for the assay. Also, negative controls yielding values lower than mean values may not be beneficial in ensuring robust assay performance.
If possible, negative control ADA samples must belong to treatment-naive subjects with the same target medical condition. Moreover, the ADA study subjects must include similar age and gender participants and participants on concomitant medications so that it adequately represents the study population. Besides, control ADA samples must be similarly collected and handled as any difference in these pre-analyte elements may influence assay results.
Development Of ADA Confirmatory Assay
As screening assays detect antibodies binding to the therapeutic drug at a pre-defined false positive rate, the US FDA recommends developing confirmatory assays to confirm antibodies binding to the therapeutic protein. A thoroughly developed ADA confirmatory assay ensures that the false-positive data does not impact the safety and efficacy of a drug product.
Selection of Format for Confirmatory Assay
The confirmatory assay format may be different or identical to the screening assay format. Usually, both these assays employ similar methods and instrument platforms. However, one must ensure assay sensitivity by determining sensitivity in mass units and confirming it through system suitability controls. Also, it becomes crucial to must optimize the competing product concentrations for verifying antibodies during binding competition assays.
Cut-Point of Confirmatory Assay
For determining cut-points for a competitive inhibition format, it is essential to assess the signal generated by samples of antibody-negative treatment-naive participants with the competitor. Usually, the competitor is the therapeutic drug, and the cut-point, in this case, must be similar to the amount of drug that will be employed in the ADA titer assay. However, ADA samples with pre-existing antibodies will require a different approach. Here one will need to exclude true positives from the assessment. Also, in the absence of baseline negative samples, one may employ an orthogonal strategy or assess changes in the ADA titer.
Clinical Vs. Preclinical ADA Assay
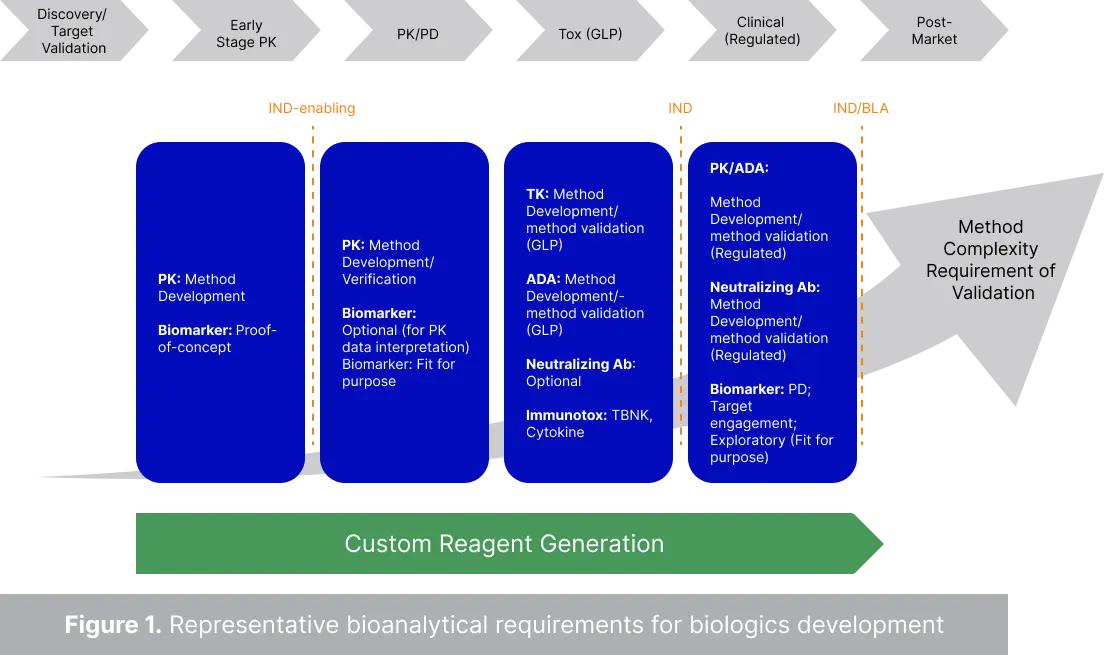
Initial preclinical studies do not require method validation, as most bioanalyses at this stage do not need GLP compliance. However, IND-enabling studies have specific method qualification and validation requirements, including ADA titer assays. These studies also include ADA assays and toxicokinetic analysis. Once the molecule advances to the clinical phase, ADA and pharmacokinetic assays will require full assay validation and higher sensitivity. Besides, the US FDA expects bioanalysis services to develop NAb assays for ADA-confirmed positive samples. Also, some biomarkers will require full method validation depending on their context of use.
During the preclinical stage, the total drug concentration is measured, while in the clinical phase, the focus is more on the free drug. In anti drug antibody testing, generally, it is necessary to measure the anti-whole drug antibodies for toxicological analysis. However, in the clinical phase, a drug with multi-functional domains will require one whole drug screening approach. This assay will be followed by confirmatory tests and characterization of domain-binding specificity. Besides, NAb assays are required during the clinical stage of drug development.
The positive controls follow a specific preparation in ADA assays or anti drug antibody testing. Usually, six to eight weeks are needed to produce polyclonal antibody reagents. However, in the clinical phase, anti-idiotype monoclonal antibodies are preferred for ADA PK analysis. On the other hand, molecules with multi-functional domains will need the measuring of domain-specific ADAs, which may sequentially need domain-specific positive controls for NAb and ADA assays.
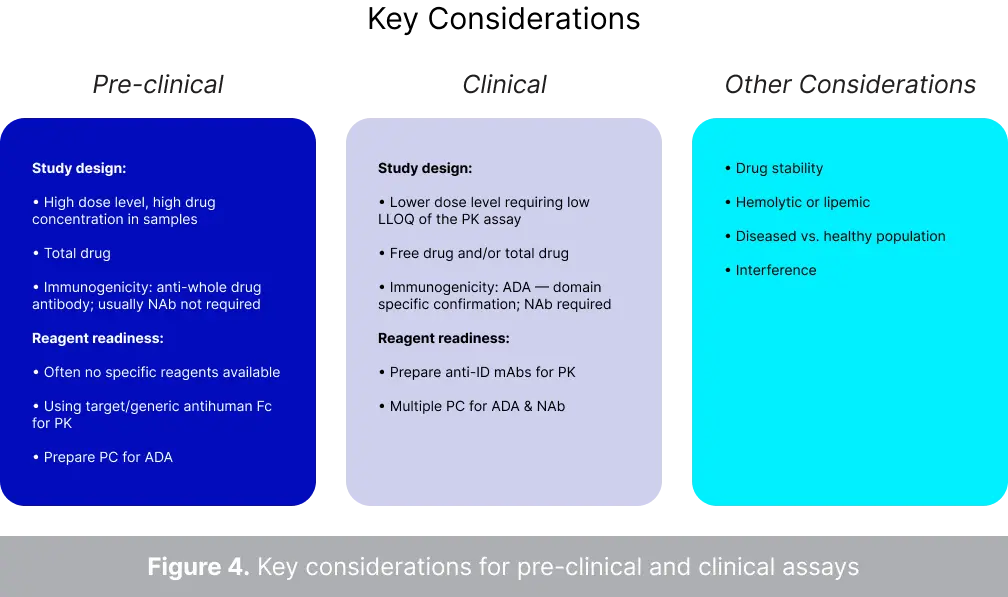
Key Considerations For Preclinical And Clinical Assays
Following is a table highlighting the crucial considerations for preclinical and clinical assays.
| Preclinical |
Clinical |
Other Considerations |
Study design:
- Total drug
- High drug concentration and high dose levels
- Anti-whole drug antibody is required for immunogenicity testing
- Generally, NAb is not needed.
|
Study design:
- Lower dose levels, hence PK assays require low LLOQ
- Determination of total and/or free drug levels
- ADA-domain-specific confirmation is needed for immunogenicity testing
- NAb is required
|
- Stable drug
- Interference
- Healthy vs. diseased subjects
- Lipemic or hemolytic
|
Reagent readiness:
- PC is needed for ADA
- Using generic or targeted anti-human Fc for PK studies
|
Reagent readiness:
- Multiple PC are needed for NAb and ADA
- PK studies require preparing anti-ID mABs
|
Inhibition Assay
Inhibition assays identify whether a secondary molecule affects drug activity. Inhibition assays are crucial during pharmaceutical drug testing as they can determine drug-drug interaction. As most medical conditions require consuming different drugs, assessing the effect of one drug product on another becomes of utmost importance.
What is the role of inhibition in drug testing?
The role of inhibition in drug testing, particularly in ADA clinical trials, is paramount for understanding the impact of drug molecules on enzymes. Assay inhibitors, such as an enzyme, modify the activity of an enzyme drug product. Enzyme inhibition assays are necessary for identifying the impact of drug molecules on enzymes. Sometimes, the cellular components interact unexpectedly, influencing normal biological processes and causing disease. Enzyme inhibitors bind to these enzymes and delay their activity, thus reducing harmful effects. Enzyme inhibition assays are also crucial for understanding disease mechanisms. For example, they can be deployed as cancer-fighting agents and help unravel oncogenic pathogenesis.
In an enzyme inhibition assay, a compound is added to an enzyme to detect inhibition. As these assays provide vital data on drug-drug interaction, clinicians rely on enzyme inhibition assay data to prescribe multiple drugs to their patients. Enzyme inhibition assays are crucial screening tools that effectively identify drug efficacy. Hence, they are vital for drug discovery and development projects and help understand how to prevent and cure medical conditions and diseases.
Executing ADA Assay Sample Analysis - Preparation And Process
FDA recommends collecting pre-treatment samples from all study subjects for ADA titer assay. As study samples may potentially have confounding components or pre-existing antibodies influencing the degree of reactivity, studying pre-treatment samples becomes crucial. Subsequent samples must be taken depending on the dose frequency of the drug product. However, one must collect samples at an appropriate time when there is minimal interference from the drug product. Besides, half-life must also be considered while deciding the sampling times.
Often thorough completion of ADA validation and cut-point determination may lead to straightforward immunogenicity testing. However, quality control and positive control samples must be assessed simultaneously with study samples. FDA recommends including quality control samples with known low, high, and negative signals. Regardless, quality control samples must be prepared in the same matrix as the study samples.
Moreover, diverse population samples will demonstrate different background activities. Likewise, if the cut-point samples are not handled similarly during assay validation and subsequent analysis, the background activity will change in ADA assays. Hence, it is essential to confirm the suitability of cut-point levels in the intended study population.
Factors Influencing ADA Responses
Although several factors discussed throughout the article will affect ADA responses, multiple other factors can influence ADA responses. These factors include therapeutic dose levels in neutralizing assay, subject-sample variability, the concentration of competing drugs, and the avidity and affinity of ADAs. Accounting for all necessary influencers is vital to analyze variability and avoid potential errors. Some other factors include pre-existing antibodies, rheumatoid factor, monoclonal antibodies, and conjugated proteins.
Additional Methods For ADA Screening
Often other methods are complemented with ADA assays. The current section discusses the three most common methods for ADA detection.
Acid Dissociation
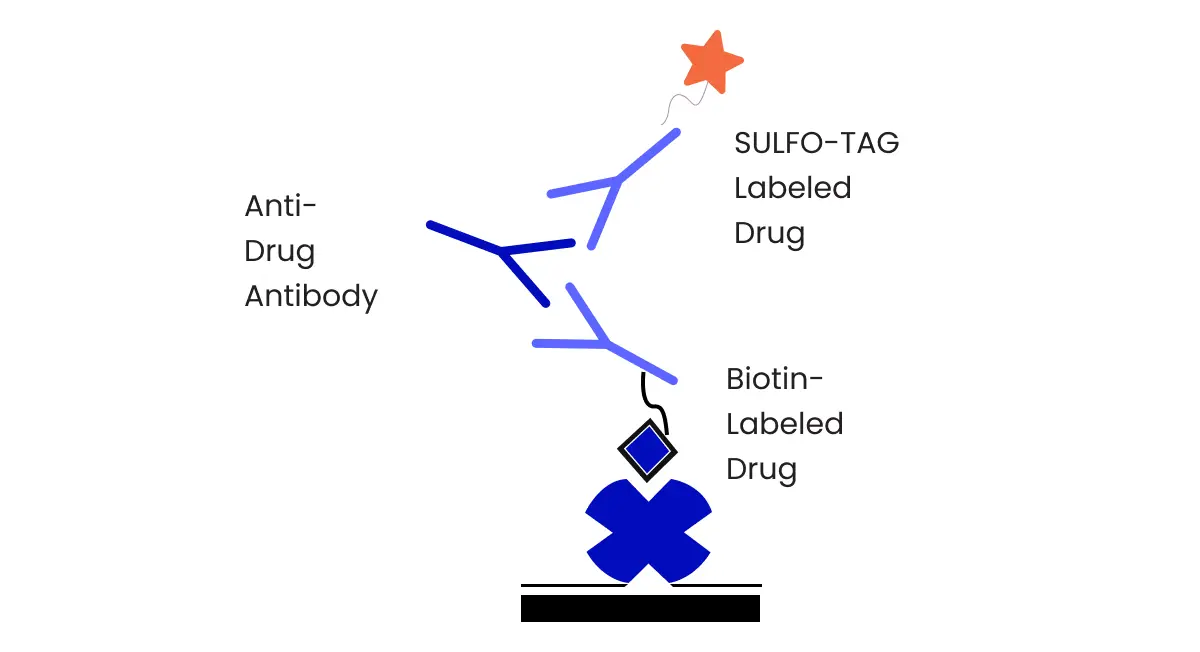
Newer sample pre-treatment methods, such as acid dissociation, are used to improve drug tolerance. This approach has drastically enhanced assay sensitivity. Today most immunogenicity testing involves ECL bridging assays with acid dissociation for lesser background noise and better assay sensitivity and drug tolerance in PK ADA Analysis.
In ECL bridging assays with acid dissociation, a biotin-labeled drug, and a Sulfo-tag labeled drug is used as capture and detection reagent respectively. ADA present in the study sample is detected because the ADA bridges both the capture and detection drug. Using bridging assays is beneficial as it determines all isotypes. Also, it is species independent and easy to perform. However, bridging assay may generate false negative results due to interference. Here, acid dissociation can help overcome the obstacle of drug interference and provide reliable results in ADA titer assay.
Solid-Phase Extraction with Acid Dissociation
Solid-phase extraction with acid dissociation helps reduce drug interference in immunogenicity assays. It is a plate-based technique that utilizes weak organic acids to dissociate the ADA-drug complex. The study sample is neutralized. It is then bound to the biotinylated drug and captured on the assay plate. The second acid treatment elutes the bound ADA, which is then transferred for a neutralizing assay. This method enhances the reliability of ADA titer assays by mitigating drug interference.
Affinity Capture Elution
Affinity capture elution is another common technique used with ELISA ADA assays. Affinity capture elution also detects circulating drug products through two acid dissociation steps. The first step disrupts the ADA-drug complex and captures the ADA on a solid surface. During the second step, the ADA is released from the complex and transferred onto a secondary transporter, and finally detected by a biotinylated drug. However, despite the advantages of the affinity capture elution step, care must be taken, as these two-step approaches may introduce anti drug antibody testing variability.
NorthEast BioLab is always ready to provide sensitive methods for robust ADA, ADA titer assay and nAb assessments. Speak to our scientists to explore the benefits of our strategies for immunogenicity testing!